Understanding Hospital Defend-In-Place Egress Strategy
December 1, 2021

By Steven Dannaway, PE, DBIA – Patients may be found in varying conditions at any given time that makes them “incapable of their own self-preservation”, including:
A Defend-In-Place Egress Strategy is the solution recognized by the building and fire codes to mitigate the hazard that fire and emergency events pose to patients in a hospital.
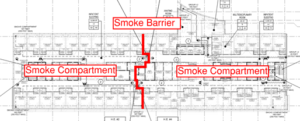 Under a Defend-In-Place Egress Strategy, hospital staff will relocate patients from the smoke compartment where the fire originates and across smoke barriers into an adjoining compartment. The adjoining compartment serves as a temporary refuge staging area for relocated patients while emergency conditions are assessed and determined if further evacuation is necessary. Visitors, ambulatory patients, and staff not involved in patient relocation can use the provided exit facilities. Patients remote from the compartment of fire origin will not evacuate and will defend-in-place.
Under a Defend-In-Place Egress Strategy, hospital staff will relocate patients from the smoke compartment where the fire originates and across smoke barriers into an adjoining compartment. The adjoining compartment serves as a temporary refuge staging area for relocated patients while emergency conditions are assessed and determined if further evacuation is necessary. Visitors, ambulatory patients, and staff not involved in patient relocation can use the provided exit facilities. Patients remote from the compartment of fire origin will not evacuate and will defend-in-place.
Total Concept
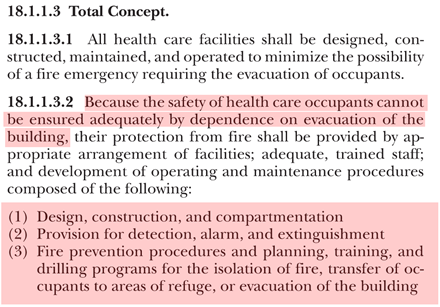
The fundamental aspects of a building that support a Defend-In-Place egress strategy are described by NFPA 101, the Life Safety Code, under a “Total Concept.”
The Total Concept involves:
The Defend-In-Place egress strategy depends heavily on a fundamental principle of fire protection engineering. This multi-faceted approach includes multiple safeguards against fire to create a safe environment for patients, staff, and visitors. Successful fire prevention and life safety strategy within a hospital facility is noted by NFPA 101, Annex 18.1.1.2 to include the following key elements:
An important item to consider as an addition to this list is the proper notification of staff on the occurrence and location of a fire event.
The International Fire Code (2021 edition, Section 403.7.2.1) and NFPA 101 (2021 edition, Section 18.7.2) require a written fire safety and evacuation plan for hospital facilities. Ultimately, it is the Owner’s responsibility to maintain such a plan and keep staff periodically instructed of their duties and responsibilities under the plan. These codes detail the minimum information that a fire safety and evacuation plan should contain.

This is a summary of the code provisions. Additional requirements may apply to your project. If you would like clarification on the healthcare code or have questions, please contact us.
Coffman is a locally driven engineering firm reinforced by a national network of multidiscipline capabilities. Our teams and processes scale quickly and move nimbly, allowing us to provide engineering solutions that are smart, practical, efficient, and have a positive impact on cost, scope, and schedule.
Contact Us
We’re entrepreneurs at heart who want to see your business and community thrive.
We draw upon our large network of talent to strive for excellence at every step.
Learn More
The right tools.
The right environment.
The right people.
Apply Now
Take a moment to review some of our news items and learn more about Coffman and our clients.
Stay Connected


