Healthcare Insights: Security Control and Means of Egress
September 27, 2021

 By Steven Dannaway, PE, DBIA – Security design is an important feature in healthcare facilities. It is common for hospital facilities to incorporate a security control system preventing unauthorized access into patient care and sleeping units, the emergency department, and operating/procedure room departments. Security requirements for a project present a unique challenge to the facility fire/life safety approach. The goals of a security system conflict with those of the means of the egress system. Security systems are intended to keep occupants out of particular areas of the building. Means of egress systems are designed to facilitate occupant access to a building’s exits and afford occupants with a path of travel to evacuate the building during an emergency.
By Steven Dannaway, PE, DBIA – Security design is an important feature in healthcare facilities. It is common for hospital facilities to incorporate a security control system preventing unauthorized access into patient care and sleeping units, the emergency department, and operating/procedure room departments. Security requirements for a project present a unique challenge to the facility fire/life safety approach. The goals of a security system conflict with those of the means of the egress system. Security systems are intended to keep occupants out of particular areas of the building. Means of egress systems are designed to facilitate occupant access to a building’s exits and afford occupants with a path of travel to evacuate the building during an emergency.
Occupants in public areas are not able to freely access their required exits when the exits are located beyond the secure perimeter. In most situations, occupants in all areas of a story require access to at least two (2) means of egress. In only a limited number of situations are areas of a building allowed to only have access to a single exit.
A Common Misconception
There is a common misconception held by designers that the California Building Code (CBC) allows required egress doors to normally be locked and to only unlock upon activation of the fire alarm system in a fail-safe mode. This is incorrect, and the building code prohibits this arrangement in many situations. Exceptions to this rule are Group I-3 occupancies (detention and correctional occupancies), Group I-2 behavioral health units (psychiatric care). Otherwise, the prescriptive requirements of the building code specify that all parts of a story must have access to at least two (2) exits with access through normally unlocked doors or doors with delayed egress locking hardware. It is not a code-compliant solution to require the egress route to pass through normally locked doors that only unlock when the fire alarm system is activated.
The permissible arrangements for door locking and access control in the means of egress are critical for designers to understand. These requirements can impact the location and arrangement of exit stairways, the security boundary, and the relationship between public and secure patient areas within a facility.
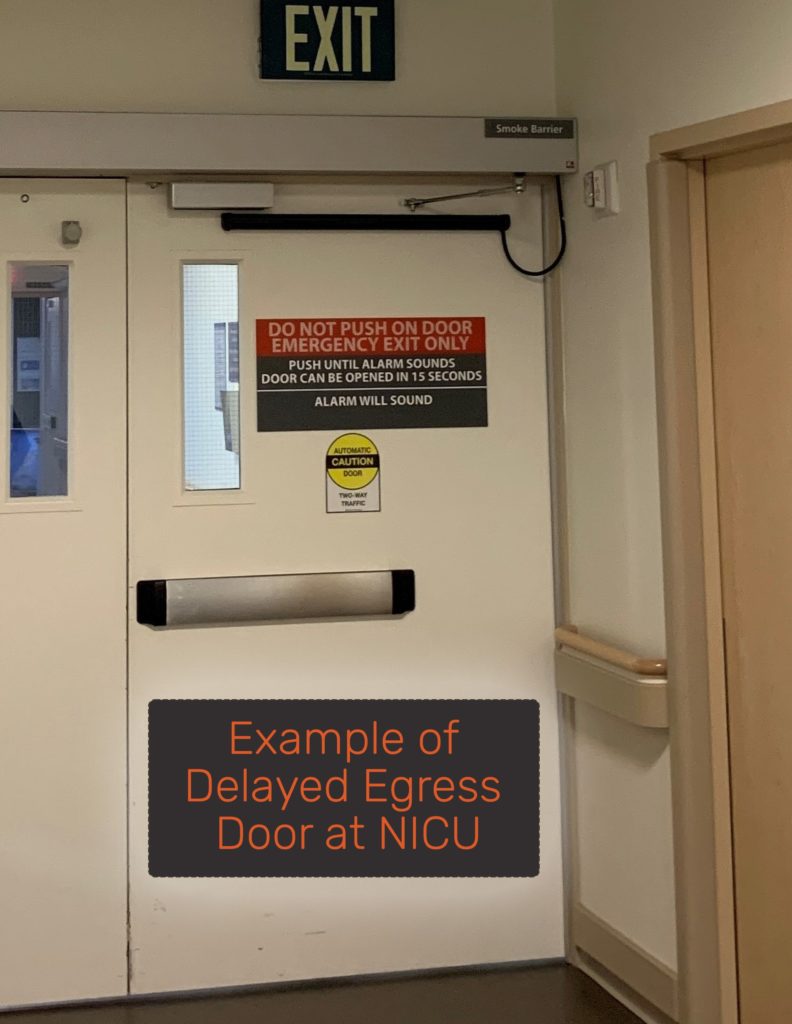
Delayed Egress Locking
Delayed egress locking hardware is a design solution; however, delayed egress doors cannot truly lock down a department. A delayed egress locking system includes hardware that will unlock after 15 seconds upon the occupant continuously applying a force to the door hardware. A local alarm is provided to signal staff in the department that the delayed egress device is being operated, allowing staff to respond to the area to verify whether an unauthorized person is trying to bypass the delayed egress door.
Consider Security Needs Early in Design
It is important early in the design phases to consider the security needs of a facility, the operations and flow of occupants between public and secure spaces, and the means of egress requirements. When the security and egress approach is coordinated early, stairs and egress paths can be defined that provide occupants in the public zones with access to their required means of egress without passing through the patient care areas. This allows the patient care units to be locked down to meet the security goals of the Owner, while also achieving compliance with the egress requirements. Failure to define the security approach early adds risk into the design process, as the means of egress approach cannot be truly defined until the location of the security perimeter is known, and increases the risk of security/egress conflicts arising down the road.
This is a summary of the code provisions. Additional requirements may apply to your project. If you would like clarification on the healthcare code or have questions, please contact us.

Coffman is a locally driven engineering firm reinforced by a national network of multidiscipline capabilities. Our teams and processes scale quickly and move nimbly, allowing us to provide engineering solutions that are smart, practical, efficient, and have a positive impact on cost, scope, and schedule.
Contact Us
We’re entrepreneurs at heart who want to see your business and community thrive.
We draw upon our large network of talent to strive for excellence at every step.
Learn More
The right tools.
The right environment.
The right people.
Apply Now
Take a moment to review some of our news items and learn more about Coffman and our clients.
Stay Connected


